HHS strives to promote the health, economic, and social well-being of children, people with disabilities, and older adults while improving wellness for all. To meet this goal, the Department is employing evidence-based strategies to strengthen families and to improve outcomes for children, adults, and communities. Underlying each objective and strategy associated with this goal is a focus on prevention.
Goal Three includes six objectives:
- Promote the safety, well-being, and healthy development of children and youth
- Promote economic and social well-being for individuals, families, and communities
- Improve the accessibility and quality of supportive services for people with disabilities and older adults
- Promote prevention and wellness across the life span
- Reduce the occurrence of infectious diseases
- Protect Americans’ health and safety during emergencies, and foster resilience in response to emergencies
Improving the Quality of Head Start Programs
The Improve the Quality of Early Childhood Education Priority Goal calls for actions to improve the quality of programs for children of low-income families, including the Head Start program. One indicator for this Priority Goal is to decrease the proportion of grantees receiving a score in the low range of the Classroom Assessment Scoring System (CLASS: Pre-K). The CLASS measures teacher-child interaction in three broad domains: Emotional Support, Classroom Organization, and Instructional Support. During the FY 2014-15 school year, 22 percent of grantees scored in the low range, thus exceeding the target of 26 percent. All grantees scoring in the low range did so for the Instructional Support domain.While smoking among adults in the U.S. has decreased significantly from a decade ago, the decline in adult smoking rates has slowed, concurrent with reductions in state investments in tobacco control programs. However, the coordinated efforts of the Agency Priority Goal to reduce tobacco use have resulted in reductions in adult cigarette consumption. The latest FY 2014 data shows that the annual per capita adult cigarette consumption fell to 1,216; missing the FY 2014 target of 1,212 by only four cigarettes. This reduction represents an approximate 9% decrease from the FY 2012 baseline of 1,342. The FY 2015 results will be available in July of 2016. The FY 2014 results of other combustible tobacco use indicators are tracking lower usage across both adults and youth:
- Percentage of adult smokers - 16.8%; exceeding the FY 2014 target of 18% (National Health Interview Survey)
- Percentage of adult smokers last smoked 6 months to 1 year ago – 7.6%; exceeding the FY 2014 target of 7.2% (National Health Interview Survey)
- Percentage of children/adolescents initiation – 3.8%; exceeding the FY 2014 target of 4.7% (National Survey on Drug Use and Health)
- Percentage of young adults initiation – 6.6%; exceeding the FY 2014 target of 7.2% (National Survey on Drug Use and Health)
These national trends and the continued plans of the Department to address combustible tobacco use make the continuation of the APG into FY 2016-FY 2017 achievable.
Salmonella is the leading known cause of bacterial foodborne illness and death in the U.S. Each year in the U.S., Salmonella causes an estimated 1.2 million illnesses and between 400 and 500 deaths. Salmonella serotype enteritidis (SE), a subtype of Salmonella, is now the most common type of salmonella in the U.S. and accounts for approximately 20 percent of all salmonella cases in humans, and reducing its prevalence is an HHS Priority Goal to reduce foodborne illness in the population. The most significant sources of foodborne SE infections are shell eggs (regulated by the Food and Drug Administration) and broiler chickens (regulated by the United States Department of Agriculture). Therefore, reducing SE illness from shell eggs is the most appropriate strategy for reducing illness from SE. Preventing Salmonella infections depends on actions taken by regulatory agencies, the food industry, and consumers to reduce contamination of food, as well as actions taken for detecting and responding to outbreaks. CDC estimated that, for 2007-2009, 40 percent of domestically-acquired, foodborne SE illnesses were from eating shell eggs and 28 percent of total SE illnesses (foodborne, non-foodborne, and international travel-associated) were from shell eggs. CDC completed an evaluation of a “food product” model to estimate annual change in percentage of SE illnesses from shell eggs, but determined that necessary data about contamination of shell eggs was not available. CDC concluded that this model could not be used unless new sources of egg data were obtained. Therefore, as of January 2014, CDC began collecting exposure data from persons with SE infection in FoodNet sites, a network that conducts surveillance for infections diagnosed by laboratory testing of samples from patients. CDC will conduct a preliminary evaluation of this data to assess its quality and determine its usefulness in updating CDC’s exposure model for estimating the proportion of total SE illnesses attributable to shell eggs during 2014-2015. As of June 2015, the SE rate was 2.9 infections per 100,000.
As part of the President’s Global Health Security Agenda (GHSA), the Office of Global Affairs (OGA) led coordination with international partners to accelerate progress toward a world safe and secure from infectious disease threats. Through this effort, the U.S. has committed to assisting 30 countries to build their capacity to prevent, detect and respond to such threats, and is partnering with over 50 countries and international organizations to strengthen health systems and to protect public health.
The 2014-15 Ebola virus disease outbreak, centered in West Africa but with global impacts and ramifications, devastated families and communities, compromised essential civic and health services, weakened economies and isolated affected populations. The outbreak also placed enormous strain on national and international response capacities and emergency response structures. HHS’s Ebola response included staff from across the Department, who worked domestically and were deployed as team members to the affected West African countries, supported the World Health Organization, Ministries of Health and other partners around the world, and undertook critical research and development domestically and overseas for new countermeasures. HHS coordinated closely with the US interagency and other governmental and nongovernmental donors, and contributed substantially to the US and global response, resulting in both control of the epidemic, and great progress in the development of countermeasures.
The Administration for Children and Families’ (ACF) Child Care and Development Fund (CCDF) program provides funding to help low-income families pay for child care and to improve the overall quality of child care programs. States continue to implement quality rating and improvement systems (QRIS) that meet benchmarks, such as providing financial support to providers and making quality information available to parents. This is also part of the Improve the Quality of Early Childhood Education Priority Goal. The number of states with QRIS that meet these benchmarks increased from 17 states in FY 2011 to 29 states in FY 2014, with FY 2015 data expected in June 2016. Targeted technical assistance provided by the new National Center on Early Childhood Quality Assurance, as well as other technical assistance partners funded by ACF, helps states work toward their goals to improve their QRIS through small group peer-to-peer interactions, national webinars, and topical learning tables related to quality benchmarks.
ACL in partnership with the Assistant Secretary for Planning and Evaluation (ASPE) developed and tested the first national, voluntary system in which states can report data collected through their APS investigations: The National Adult Maltreatment Reporting Systems (NAMRS). The most recent data on the prevalence of elder abuse, neglect and exploitation suggest that at least 10 percent or approximately 5 million, older Americans experience abuse each year. In addition, adults with disabilities are at increased risk of experiencing abuse and neglect. An absence of federal stewardship in Adult Protective Services (APS) has led to a host of challenges including inconsistent data systems and non-uniform reporting requirements that prevent APS programs from evaluating their services or conducting meaningful program evaluation. NAMRS was developed to address this challenge. The new system along with competitive grants to states to enhance state APS programs and services including reporting capacity is on track to have all states submitting data in FY 2017.
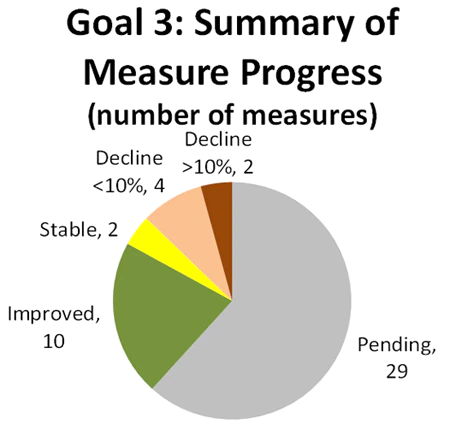
For this goal, 67 percent of measures with available data showed stable or improved performance.