Although viral hepatitis affects millions of Americans nationwide from all social, economic, and racial and ethnic groups, it disproportionately impacts certain populations and communities. Hepatitis prevention and treatment efforts can be more efficient and effective by identifying and focusing efforts on those populations that bear a disproportionately higher burden of infection and disease, referred to in the Viral Hepatitis Plan as priority populations. The Plan uses nationwide surveillance data to determine the priority populations. Focusing on the priority populations will reduce health disparities and put the nation on the path toward elimination of viral hepatitis. This approach should not diminish efforts to increase awareness, prevention, treatment, and integration of viral hepatitis efforts more generally, for all populations.
National incidence, prevalence, and mortality rates were used to identify a small number of groups most impacted by each type of hepatitis. Of note, national data on many populations are limited, and the data-driven approach of this plan to identify priority populations does not result in every population at higher risk or prevalence being included among the priority populations. For example, more information is needed at the national level on the viral hepatitis risks, incidence, prevalence, and mortality of non-U.S.-born, justice-involved, and sexual and gender minority populations. The Viral Hepatitis Plan includes strategies to improve services among these as well as other populations and to address the data gaps.
Priority Populations
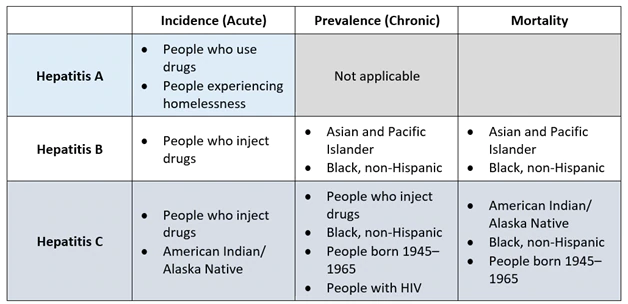
National-level data for calendar year 2018 illustrate the disparate impact of hepatitis A, hepatitis B, and hepatitis C (see Table below). Additional data are available in CDC’s Viral Hepatitis Surveillance—United States, 2018 and are posted on CDC’s website as they become available. This report is the source for all data cited below unless otherwise specified.
Priority Populations and Summary National-Level Data
Calendar Year 2018 (unless otherwise indicated)
|
People Who Use and/or Inject Drugs
|
|---|
- Hepatitis A outbreaks have sickened more than 30,000 people across the United States since 2016; 26% of outbreak-associated patients in California, Kentucky, Michigan, and Utah are homeless and use drugs.
- Among reported cases with IDU information available, 50% of hepatitis A, 36% of acute hepatitis B, and 72% of acute hepatitis C cases report IDU.
- The rates of acute hepatitis B and acute hepatitis C cases are highest among age groups most impacted by the nation’s opioid crisis (aged 30–49 years for hepatitis B and aged 20–39 years for hepatitis C).
|
|
People Experiencing Homelessness
|
|---|
- People experiencing homelessness comprise a large proportion (33% in outbreaks in California, Kentucky, Michigan, and Utah in 2017) of people infected during the person-to-person hepatitis A outbreaks starting in 2016.
|
|
Asian and Pacific Islander (API)
|
|---|
- Asian Americans account for 58% of Americans living with chronic hepatitis B but comprise only 6% of the total U.S. population. The prevalence of chronic hepatitis B among non-Hispanic Asians (3.41%) was 31 times the prevalence among non-Hispanic whites (0.11%).
- API had a higher hepatitis B–related mortality rate (2.1 per 100,000) compared to non-Hispanic whites (0.27 per 100,000).
|
|
Black, Non-Hispanic
|
|---|
- Non-Hispanic Blacks had a higher hepatitis B–related mortality rate (0.7 per 100,000) compared to non-Hispanic whites (0.27 per 100,000) and a higher hepatitis C–related mortality rate (6.31 per 100,000) compared to non-Hispanic whites (3.35 per 100,000).
- African immigrants account for approximately 12% of all Americans living with chronic hepatitis B. The prevalence of chronic hepatitis B among non-Hispanic Blacks (0.69%) was more than 6 times the prevalence among non-Hispanic whites (0.11%).
- Among people aged 20–59 years and 60 years or older, non-Hispanic Blacks were more likely [Odds Ratio (OR)=1.6 (CI: 1.1, 2.3) and OR=10.0 (CI: 4.9, 20.1), respectively] to have chronic hepatitis C than all other race/ethnicities.
|
|
American Indian/Alaska Native (AI/AN)
|
|---|
- The incidence rate of acute hepatitis C among AI/AN has remained substantially higher than other racial/ethnic populations from 2003 to 2018. In 2018, the rate of incident acute hepatitis C was higher among AI/AN (3.6 per 100,000) than among non-Hispanic whites (1.3 per 100,000).
- The age-adjusted, hepatitis C–related mortality rate among AI/AN has been higher than all other racial/ethnic populations since 2013. The mortality rate among AI/AN was 2.7 times the rate among non-Hispanic whites, 1.4 times the rate among non-Hispanic Blacks, 2.0 times the rate among Hispanics, and 6.3 times the rate among APIs in 2018.
|
|
People Born from 1945 through 1965
|
|---|
- Approximately 75% of people with chronic hepatitis C were born from 1945 through 1965.
- People aged 55–64 years and 65–74 years (19.7 per 100,000 and 14.8 per 100,000, respectively) had higher mortality rates than any other age group.
|
|
People with HIV
|
|---|
- Among people with HIV who also inject drugs, 62–81% were coinfected with hepatitis C.
- Among people with HIV in 15 U.S. states and two cities, 6.7% were coinfected with hepatitis C.
- HIV patients coinfected with hepatitis B or hepatitis C have higher liver-related morbidity and mortality, as well as higher overall mortality, than patients only infected with hepatitis B or hepatitis C.
|
Learn more about the Viral Hepatitis Plan or download the plan to read it