

Real-Time Decision Support at the Intersection of Public Health and Health Care
Executive Summary
 The Center for Disease Control and Prevention’s (CDC) National Center for Chronic Disease Prevention and their State partners devote resources to manage and control chronic disease: largely preventable conditions that are responsible for 7 of every 10 U.S. deaths and account for more than 75% of the annual $2.5 trillion in U.S. medical care costs. Public health monitoring is vital in measuring both the need and effects of initiatives that target the most vulnerable patient populations.
The Center for Disease Control and Prevention’s (CDC) National Center for Chronic Disease Prevention and their State partners devote resources to manage and control chronic disease: largely preventable conditions that are responsible for 7 of every 10 U.S. deaths and account for more than 75% of the annual $2.5 trillion in U.S. medical care costs. Public health monitoring is vital in measuring both the need and effects of initiatives that target the most vulnerable patient populations.
In recent years, a new source of data has emerged that has the potential to provide unprecedented depth of local population health information, enabling greater insight into patterns of care and the ability to strengthen decision support around care delivery. As Electronic Health Records (EHRs) become the standard of care for medicine, public health needs to continue developing relationships with health care systems to successfully leverage these resources to enhance monitoring and interventions. This project serves as an example of how this type of collaboration can be developed and sustained.
Each day, between 10-20% of patients in the United States do not arrive for their outpatient appointments. At The Emory Clinic in Georgia, this represents hundreds of patients per day, a missed opportunity to deliver care and an annual revenue loss of millions of dollars. Healthcare systems are able to overbook patient appointments to offset the revenue risk, but robust decision support tools do not currently facilitate the differentiation between patients who are at increased risk of poor health outcomes due to missing their scheduled care. The ability to differentiate patients who are healthy and stable from those who are at increased risk of poor outcomes and diminishing health will be critical in directing finite resources towards best managing populations.
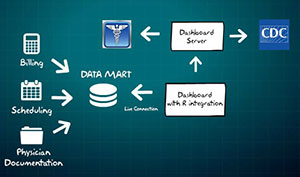
The Innovation: This project explores ways to transfer and combine EHR and contextual population level data to create robust data visualization tools that will help support decision-making and resource deployment for both public health and health care organizations. This data will be used to determine no-show risk propensity and health stability scores for patients and communities.
By identifying patients who are both at risk for missing appointments and having negative health outcomes, health care systems can better direct finite resources towards best managing their patient populations. Moreover, by identifying segments of the community that have potential access to needed care but are not utilizing it, public health systems can proactively identify, and then prioritize and evaluate, outreach efforts to overcome the barriers to care these groups face.
A project supported by the: HHS Ignite Accelerator
Team Members
Matthew Ritchey (Project Lead), CDC/ONDIEH
Linda Roesch, CDC/ONDIEH
Sarah Kier, The Emory Clinic
Alan Kramer, The Emory Clinic
Milestones
May 2014: Project selected into the HHS Ignite Accelerator
June 2014: Time in the Accelerator began
September 2014: Time in the Accelerator ended
Project Sponsor
Michael Schooley, Branch Chief, Division for Heart Disease and Stroke Prevention, Office of Noncommunicable Diseases, Injury and Environmental Health (ONDIEH), Centers for Disease Control and Prevention (CDC)
Joseph John, Vice President of Operations, The Emory Clinic; Assistant Dean for Administration, Woodruff Health Sciences Center
Greg Esper, Director of New Care Models, Emory Healthcare; Vice-Chairman for Clinical Affairs, Department of Neurology