



U.S. Department of Health & Human Services
Health Resources and Services Administration
HRSA Press Office: (301) 443-3376
by HRSA Administrator Mary K. Wakefield
January 13, 2011
Washington, D.C.
I’m happy to be with all of you today. I was pleased to accept your invitation to explain HRSA’s role in health and health care and hopefully, in the process, spark thinking about where our agendas might align and how we can – in partnership – be more effective and efficient in deploying our respective resources.
By way of background, HRSA is one of 11 agencies within the U.S. Department of Health and Human Services. Many of our sister agencies – FDA and CDC – for example, have higher public profiles than ours, so I often begin speeches by explaining what it is that we do.
HRSA is often called the “safety-net agency,” or the “access agency,” because our role is to expand access to quality health care in medically underserved communities and populations. We do that by awarding funds to state, local and community-based organizations that deliver health care and services, and by overseeing the work that they do.
Put differently, there is almost nothing that HRSA does that it does alone. Virtually everything we do is done in partnership with organizations from community to national levels and all points in between.
HRSA manages 80 different grant programs:
- In our Community Health Center system, we have 1,100 grantees that provide primary and preventive care at more than 7,900 clinical sites across the nation. They exist in each of your states and the territories. This network, which will expand dramatically over the next several years, served nearly 19 million patients in 2009 at an average annual cost of about $600 per person. That’s extremely cost-effective by any measure; I’ll come back to this program in a couple of minutes.
- HRSA also administers the Ryan White HIV/AIDS Program, whose 900 grantees provide top-quality care and life-sustaining medication to more than half a million low-income and uninsured people living with HIV/AIDS. That’s half of all Americans who’ve been diagnosed.
- Next, our Maternal and Child Health block grants to states pay for health care services, screening and counseling that reach six of every 10 women in the U.S. who give birth, and their infants. Within this effort, we also target resources to high-need areas – our Healthy Start program is in more than 100 communities with high infant mortality rates.
- HRSA also manages the National Health Service Corps, which places primary care professionals in medically underserved areas in exchange for student loan repayments and scholarships. We currently support about 7,500 of clinicians in the field, but many, many more are on their way because of the Recovery Act and the Affordable Care Act.
- Similarly, HRSA strengthens the nation’s primary care workforce by giving financial support to colleges and universities for training and curriculum development, and for scholarship and loan repayment programs for health professions students.
- We also house the Department’s Office of Rural Health Policy, which bolsters rural hospitals and coordinates coalitions of rural providers. Nearly 7 out of 10 health professions shortage areas nationwide are in rural communities, and HRSA is the lead federal agency in helping them come up with solutions to health care scarcity.
- In addition, HRSA promotes and supports the expanded use of telehealth to connect underserved people to distant providers through remote monitoring devices and teleconferencing. This is especially crucial in rural and remote parts of the country, where care providers historically have been few and far between.
- Finally, HRSA oversees the nation’s Poison Control Centers; our federal organ procurement and allocation efforts; and the National Vaccine Injury Compensation Program, among other programs.
HRSA’s vision as an agency is focused on Healthy Communities and Healthy People. Our mission is: to improve health and achieve health equity through access to quality services, a skilled health workforce and innovative programs. It’s a tall order, but one we’re committed to through our strategic plan and associated work.
- Our strategic plan has four goals. The first is to improve access to quality health care and services.
We’re doing this, in part, by assuring a medical home for the populations our grantees serve; by expanding oral health and behavioral health services and integrating them into primary care settings; and by integrating primary care and public health.
- Our second goal is to strengthen the health workforce.
We’re using our programs to train the health workforce to provide high quality, culturally and linguistically appropriate care; to increase the number of providers to address shortages; and to develop strategies to monitor, forecast and meet long-term health workforce needs.
- Goal number three is to build healthy communities.
Here, we collaborate with others to help communities strengthen resources that improve health for the population. Part of our efforts focus on linking people to services and supports from other sectors that contribute to good health and wellbeing, and we’re focused on strengthening illness prevention and health promotion efforts across populations and communities. More broadly, that’s a focus of the ACA.
- Our fourth goal is to improve health equity: we want to eliminate disparities in access to quality health care across populations and communities.
To do that, we’re working to identify and advance evidence-based and promising practices to achieve health equity. And we are partnering with diverse communities and diverse organizations to develop and disseminate innovative community-based health equity solutions, with a particular focus on populations with the greatest health disparities.
As I alluded to earlier, only by building partnerships can HRSA meet our goals, and that’s part of the reason why I was happy to accept the invitation to speak with you today.
And from what I’ve read online about NACo positions on health reform, I think we have many of the same goals. NACo supports a greater focus on prevention and access to care and greater efforts to recruit and train health professionals. At HRSA we are busy implementing aspects of the Affordable Care Act that deal with precisely those issues. In fact, HRSA has the lead in implementing more than 50 provisions in the legislation, and is the co-lead in over a dozen more.
So in many ways, HRSA and county organizations are natural partners.
HRSA has resources we’d like you to know more about, because we want you to be in the position to access them. Resources have come to us through the Affordable Care Act and the Recovery Act to supplement key programs that we administer as part of our regular annual appropriations. And online, we have a wealth of health information at the county level that officials may want to consider when making local health investments.
Let me begin my overview of the resources at HRSA that counties may want to know about and access by focusing on the sizable support we received through the Affordable Care Act for health centers and the National Health Service Corps.
These investments are designed to improve access to primary care and preventive services, and encourage health care professionals to serve where they are needed most.
Through the ACA, HRSA will administer $11 billion over the next five years to expand health center sites and services. This investment will nearly double the current patient base of 19 million.
As I noted at the beginning of my remarks, HRSA supports almost 8,000 health center sites across the United States. The number of those sites will grow as we add new grantees through the ACA. And the physical size of those sites and the range of services they provide will grow.
If you have federally qualified health centers in your county, make sure they are aware of the opportunities that await them to expand their services. If some parts of your communities are medically underserved and eligible to apply to establish a health center, there are and will be competitions to select new grantees.
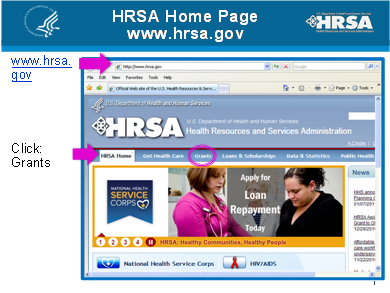
There are several ways you can make sure you or your partners stay up-to-date on grant opportunities. The easiest way is to go first to the HRSA website at www.hrsa.gov, and click on “Grants” at the top of the page.
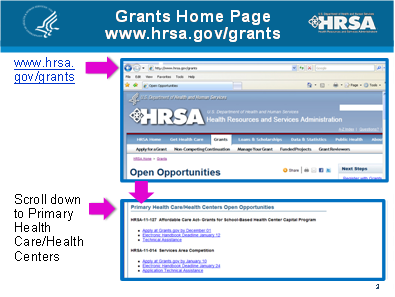
Once you move to the Grants home page, scroll down from the “Open Opportunities” header until you see “Primary Health Care/Health Centers.” Click there and all the current grant opportunity for health centers will be listed.
If you want to talk to someone live, call our staff in the Bureau of Primary Health Care, which administers the health center system.
Or you can call your state Primary Care Office; those are organizations HRSA funds whose job is to increase access to health care for underserved populations in their states. You can find your state PCO online at the HRSA website: just type in “PCO” in the search box and the entire national list will pop up as your first choice.
Additionally, you can contact HRSA’s Regional Offices. There are 10 HRSA regional offices throughout the country, and they are there to help you. I urge you to make them your friends in your region. To help you do that, I brought handouts for all of you with the names of our Regional directors, building addresses, phone numbers and email addresses.
Our staff, whether in the Regional Offices, in the Bureau of Primary Care or in the rest of HRSA’s operations, are there to answer your questions and help you in whatever you seek. So please, use them! If you don’t get the response you’re looking for – call or email me.
Let me add in another angle here that is worth underscoring. That is that health centers are not only vital contributors to the health of local residents, they are also generators of a substantial number of local jobs, especially in rural areas.
HRSA-supported studies by the Center for Rural Health Works at Oklahoma State University show that a hospital or health center in a small town is often the second largest employer.
In private practice, a typical rural doctor hires a nurse, a medical technician and a receptionist. And referrals by that doctor to the local hospital also support jobs there as well.
So the existence of a health center not only leads to healthy people, it also helps contribute to economically healthy communities. And that, as I said earlier, is HRSA’s vision for America.
Now let me turn to the second major program I wanted to spend a minute on, the National Health Service Corps.
HRSA will administer $1.5 billion in Affordable Care Act dollars through 2015 to expand the number of NHSC clinicians working throughout the country in medically underserved areas.
For those of you unfamiliar with the NHSC, the Corps offers newly graduated advanced practice nurses, dentists, doctors and other health care professionals $60,000 in loan repayments for a two-year commitment to work in needy areas. That sum can be extended to $170,000 for a five-year commitment. Loan repayments are tax-free.
The ACA dollars follow an investment of $300 million in the NHSC from the Recovery Act of 2009. We have added thousands of clinicians to the NHSC’s ranks in the past couple of years after years of anemic funding.
The NHSC just opened its most recent Loan Repayment application cycle in late November. We expect to issue the first of these awards later this month. The point I’m making is that we have more NHSC clinicians available to work at eligible clinics than ever before.
And the NHSC website, which can be accessed, of course, through the HRSA home page, has a wealth of information about which clinics are looking for NHSC loan repayors, or how clinics can qualify to hire clinicians if they haven’t already. This is a program that can assist kids from your counties and health facilities in your counties.
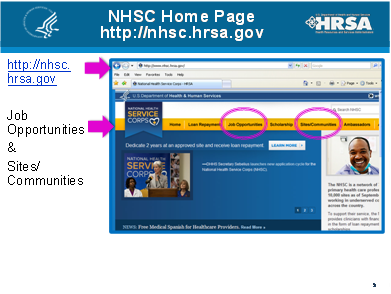
Click on “Job Opportunities” at the NHSC site and you can see clinics listed by county that are hoping to attract NHSC loan repayors. I encourage you to take a look at the list; chances are that a clinic in your county is advertising here for an NHSC clinician. We’re also working through our PCO offices to get more eligible sites designated. Maybe you know someone who knows someone who’s looking for just that kind of opportunity to make a difference. Maybe you can spark that connection. You never know!
In other words – now that you know what a great deal the NHSC is – maybe you want to learn how to qualify a worthy clinic in your county to hire an NHSC clinician. Just stay on the NHSC website; this time click on “Sites/Communities” and you’ll be led through the qualification process.
Or, again, call your state Primary Care Office; it’s their job to help you through the process. HRSA staff in our Bureau of Clinician Recruitment and Service also can help you; they run the NHSC program. Or contact your new friends in the HRSA Regional Office.
Now let me shift gears a bit and tell you about three online sources county officials can turn to for free health-related and demographic information at the county level. The first is a HRSA site, the second a HRSA-supported product on an HHS site, and the third is a joint foundation-university product.
This is the home page of the Area Resources File that HRSA maintains.
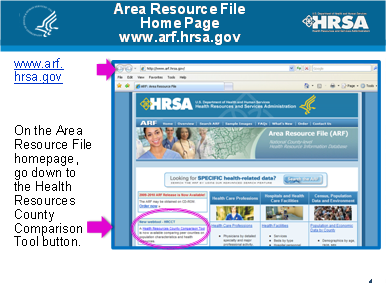
Look at the left side of the page and you’ll see a new web tool – the Health Resources County Comparison Tool. Click there and you’ll be able to bring up data by county on population characteristics and health resources, such as the number of doctors and dentists, along with the number of hospitals and health centers.
You can compare your county’s performance to those of a number of “peer counties” with similar demographics that are selected by the software. You also can compare your county to up to three counties of your choice, if you want to see how your neighbors are doing. The tool gives you a good snapshot and it’s easy to use.
The second free county-based resource is the Community Health Status Indicators website.
HRSA was a major contributor to the CHSI site, which contains demographic information and a broad compilation of statistics on birth and death rates in all U.S. counties. The site also lists per county counts on infectious diseases, use of preventive services, and risk factors for premature death.
The CHSI site also is easy to use. Many of the tables have a comparison column that gives a county an “apple” icon if its status is favorable to that of its peer counties in, say, births to women under 18, infant mortality, or breast cancer rates. On the other hand, if a county’s status is below the average for its peers, the column switches out the apple for a “microscope” icon, indicating that closer attention needs to be paid to that issue.
Additional health information by county is available at www.countyhealthrankings.org. That’s not a federal site; it’s a product of the Robert Wood Johnson Foundation and the University of Wisconsin, but it also contains useful free information for county officials.
Before I close, I’d like to tell you about a brand-new initiative, funded by the Affordable Care Act, that we’re hoping counties and local health departments will join.
Late last year, we announced a grant to a Boston nonprofit to establish a Healthy Weight Initiative. Beginning in March the initiative will begin to organize teams in all 50 states to implement and test a set of evidence-based interventions designed to reduce obesity.
The National Association of County and City Health Officials is already onboard as a partner of our grantee in the initiative. Look for more information on it in coming months.
We do hope that local health departments will join their state teams in this important endeavor. And I hope that counties will join us not only on that initiative but in the ongoing work I’ve described today.
I recently did an interview for the December newsletter of the National Association of County Behavioral Health and Developmental Disability Directors, and I reiterated my hope that counties will partner in greater numbers with local HRSA grantees.
I told Ron Manderscheid, who leads the National Association, that increasing these partnerships will require HRSA to brief county officials about who these grantees are, where they are located, and what they are trying to accomplish. I hope that I’ve been successful in beginning that dialogue here today with all of you.
At HRSA we welcome input from county officials on what we’re doing at HRSA. If your members have ideas on what we can do better, please let us know. I mean that. We’re about performance improvement in what we do and how we do it, and we’re open to good ideas wherever we find them.
I hope you’ll leave here today with knowing that HRSA programs are implemented, in the main, at the local, community level. We have assets that cities, counties and communities use to improve the lives of their residents. We collect data at the county level and we focus on your world. Because of the focus of HRSA’s mission, counties matter a great deal to us, and they certainly matter to me.
Thank you for inviting me here today.






